URI experts plot a vaccine’s progress from laboratory to pharmacy.
It is November 24, 2020, and the United States is reporting 12.5 million cases of COVID-19. More than a quarter of a million Americans have died of the virus.
Hospitals and their medical staff are strained to an alarming rate and epidemiologist Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota and a member of President-elect Joe Biden’s coronavirus advisory board, warns of a dangerous winter ahead as COVID-19 cases multiply exponentially.
A bright spot in this ominous forecast: The pharmaceutical companies Pfizer and Moderna report they’ve developed vaccines with efficacy rates of 95 percent. AstraZeneca has also announced a vaccine. And more pharmaceutical companies continue to work on still other vaccines.
There are close to eight billion people on the planet, and 328 million of those are United States citizens.
So how will a global inoculation happen? We asked four URI experts: Alan Rothman, Kerry LaPlante, Koray Ozpolat, and Virginia Lemay, to discuss how a vaccine is developed, evaluated for safety and efficacy, manufactured, and administered.
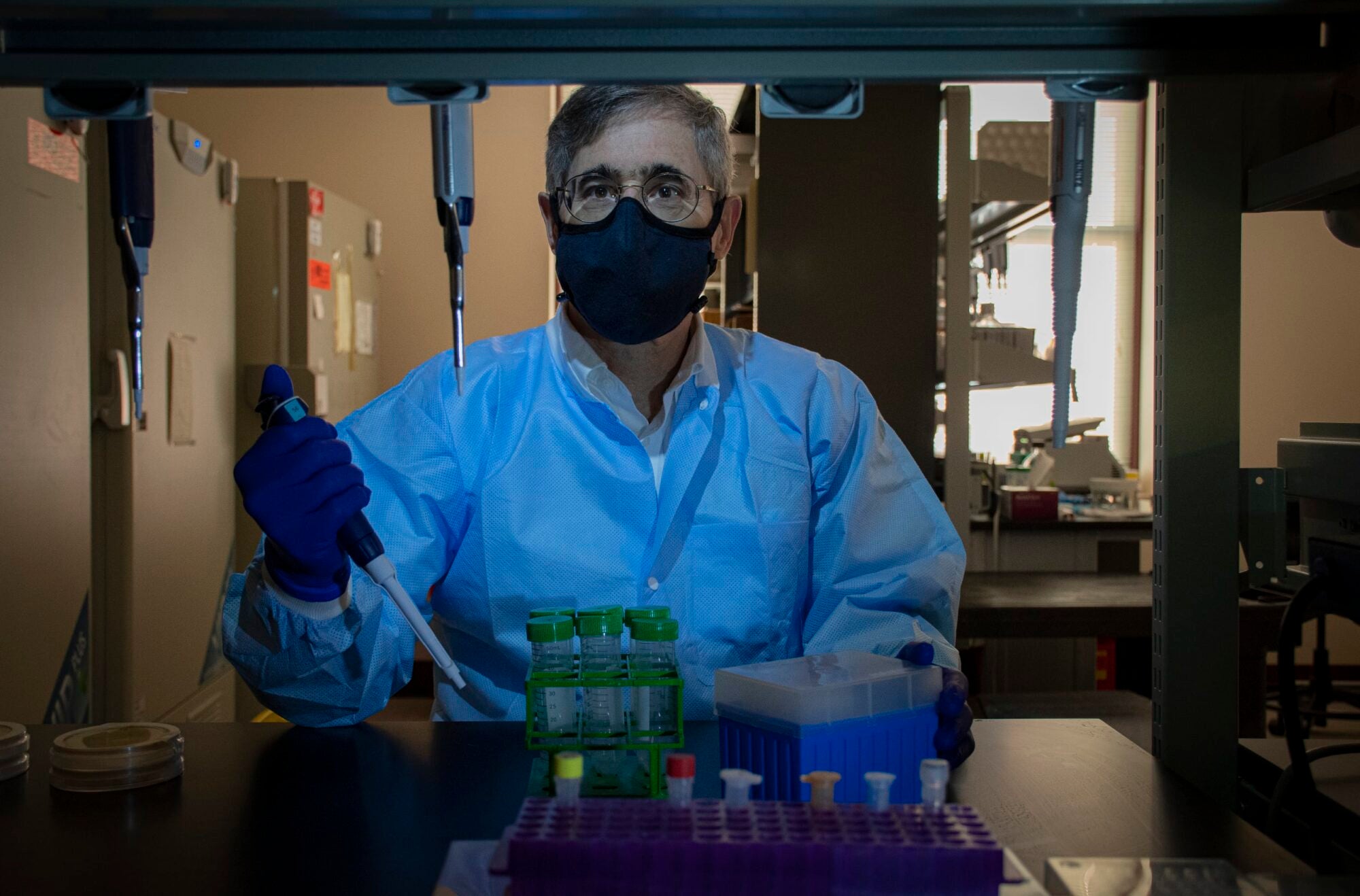
Dr. Alan L. Rothman in his lab
Creating a vaccine
A vaccine enables a body’s immune system to fight disease. In effect, the vaccine trains the immune system to detect and defend against intruders: viruses and bacteria, preventing sickness. The process of developing and bringing a vaccine to market can take years because of the lab testing and clinical trials involved.
Vaccines are made by taking viruses or bacteria and weakening them so that they can’t reproduce or replicate. There are four approaches to creating a vaccine:
- Change the virus blueprint or genes so that the virus replicates poorly.
- Destroy the virus blueprint so it can’t replicate itself at all.
- Use only a part of the virus or bacteria.
- Take the toxin released from the bacteria, purify it, and kill it.
And likely add a booster shot.
In the case of COVID-19, the research and development process has been accelerated, but that hasn’t been at the expense of basic safety protocols. Three phases of clinical trials must be successfully completed before the federal Food and Drug Administration will license a vaccine. Success is measured in terms of its safety and efficacy and an assessment that the vaccine’s benefits outweigh its risks.
In the first phase of a typical clinical trial, a small pool of people, between 20 and 100 volunteers, are vaccinated. In the second phase, that group of volunteers is extended to several hundred people. And in the third phase, the number of volunteers is in the five figures, 60,000-plus.
The research and development phase of a vaccine can take years, says Dr. Alan L. Rothman, research professor and head of URI’s Laboratory of Viral Immunity and Pathogenesis. Dr. Rothman is developing a vaccine for dengue fever, a mosquito-borne virus that infects more than 400 million annually in over 100 countries worldwide. About 100 million infected get sick and, of those, 22,000 die annually. “Dengue” is an umbrella term for four related viruses; conceivably, a single individual can contract the virus up to four times in their lifetime.

Dr. Rothman has been researching the disease for more than 30 years seeking answers to questions about transmission, susceptibility, and long-term effects. “It’s the features of dengue that make it interesting” in relation to COVID-19, Dr. Rothman says. “There are a lot of instructive parallels. For instance, the disease can happen more than once. Hundreds of millions get it.”
Sound familiar?
In a 2015 60 Minutes interview Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Disease, was asked what kept him up at night. His answer: “An influenza-like respiratory-borne virus that’s easily transmittable to which the population of the world has very little if any immunity against and that has a high degree of morbidity and mortality.”
COVID-19 checks all the boxes.
Media outlets have reported that a vaccine rollout could begin early in the new year. Dr. Rothman says he will delve into the data to determine when the vaccine is the right choice for himself and his family. He monitors how much transmission is going on in his community. “And I rely on information coming out of the Centers for Disease Control and the NIH,” Dr. Rothman says. “I take into account my own feelings and other sources.”
And he considers the lessons of the past.
“Some vaccines are unhelpful and some detrimental. A vaccine can make things worse,” Dr. Rothman says. “As a researcher, you are sobered by the fact that you can make things worse.
“There is a threat in a rush to market, and there is a threat in delay,” he explains. “We’re trying to balance those things.”
In the meantime, Dr. Rothman’s advice aligns with Fauci’s to reduce transmission of the virus: Wear a mask. Wash hands frequently. Limit interactions. Practice physical distancing. “The goal is to decompress the disaster our health care systems could face,” Dr. Rothman says. “We don’t want it to spread around because we can’t afford to have all those people going into intensive care at the same time.
“Coronavirus is ahead of us now. I’m hopeful it doesn’t have any special tricks up its sleeve. I’m hopeful of finding a vaccine that will work,” Dr. Rothman says. “How long will it work is another question. We can’t afford to make things worse. A 1% mortality rate even is a horrible thing, but what if we make it 1.5? Even a low risk of side effects could involve a lot of people.”
That said, Dr. Rothman is heartened by the progress made toward a vaccine.
“Any time a vaccine is tested, you’re hopeful.”

Professor Koray Özpolat at the College of Business
‘A massive endeavor’
What does it take to bring a vaccine to market on a global scale? Supply chain management plays a crucial role, says Koray Özpolat, an associate professor and coordinator of the doctoral program in supply chain management in the College of Business.
“Ensuring success relies on a well-coordinated end-to-end vaccine supply chain, which consists of three stages; sourcing, manufacturing, and distribution,” says Özpolat.
Initially trained as an electrical engineer, Özpolat’s interest in humanitarian logistics and disaster relief developed when he was a logistics systems analyst for the United Nations. He provided process mapping and programming support to the Procurement and Logistics Division. This work led Özpolat to earn a Ph.D. in supply chain management and conduct research on how to improve humanitarian supply chains.
“In bringing a vaccine to the market, typically sourcing, manufacturing, and distribution is a sequential process,” Özpolat says. “One stage depends on the successful execution of the prior stage.”
And then, there is the need to account for lead time. For example, to be ready for flu season, which spans October to January, the distribution of influenza vaccine to clinics and pharmacies starts in late summer. Sourcing and manufacturing of the vaccine begin eight months before distribution, Özpolat says. So the whole process typically amounts to a full year after the vaccine is approved.
Capacity is another challenge.
“We’re looking to gear up and run supply chains on a scale not seen in the pharmaceutical industry, and we will have to do these in parallel with all immunizations already in place,” Özpolat adds. “It’s a massive endeavor involving the pharmaceutical industry, suppliers, logistics companies (such as FedEx), and federal and local governments to build sourcing capabilities, manufacturing capacity, and proper distribution channels and shrink what is normally a one-year cycle into months.”
Özpolat notes that there has been unprecedented collaboration between competitors and across business sectors to be ready for the global distribution of a vaccine or vaccines. Companies and government agencies are divvying up and attending to challenges such as how to mass-produce hundreds of millions of glass vials. UPS is growing its healthcare logistics division.
“Even the Department of Defense is ready to weigh in if more distribution is needed,” Özpolat notes. “In the United States, we will need more than 500 million doses of COVID vaccine. While each state will decide how to administer their COVID-19 vaccine program, early doses will probably go to front-line workers and at-risk citizens.”

There is the risk of the first vaccine not being the best one, for example. The supply chain will have to be flexible enough to pivot to a new vaccine, Özpolat explains. Another challenge supply chain management must anticipate is sourcing competition on a global scale. Demand for certain ingredients could cause a crisis of global scarcity. For instance, Tamiflu, a drug used to treat avian influenza, contains an extract from the star anise, which grows in an area southwest of China, Özpolat notes. If a coronavirus vaccine requires ingredients from plants that are not easily cultivated or which grow only in specific parts of the world, global competition could ensue. Extraordinary demand for ordinary products such as syringes or glass vials could create a scarcity issue.
“COVID-19 is a global problem, and none of us will feel safe until all of us feel safe,” Özpolat says. “It is funny how a man allegedly eating a soup of wild animals in China resulted in toilet paper shortages in America two months later. This shows not only how connected humanity is but also how fragile global supply chains can be.
“Countries should look for more ways to cooperate globally,” Özpolat adds. “Pfizer’s COVID-19 vaccine project is conducted jointly with the German company BioNTech. American Pfizer’s Greek CEO Albert Bourla and the German BioNTech’s Turkish CEO Ugur Sahin work together and demonstrate a perfect example of this global cooperation.”
Özpolat is also optimistic at the industry collaboration he’s seen around readying for a vaccine. “Normally what would take a year is being done in a month now. Everyone is working on a different level.”
Acceleration should not provoke anxiety, necessarily, he says. “It’s partially prioritization. Companies are moving more human resources onto COVID. And there’s the money to turn the sequential vaccine development process into a parallel one and shave off many months from the year-long lead time.
“Normally, government approvals are needed. Vetting takes time. The government is moving faster now,” he adds. “Suspecting political influence on approval, many Americans may hesitate to take the vaccine, but I trust the integrity of the pharmaceutical industry. Companies have agreed not to release the vaccine until they are sure it’s safe and effective. The industry is checking on each other, and I feel confident to line up outside a CVS to receive the vaccine once it’s available.”
That is not to say Özpolat will not be scrutinizing the entire process. “As an academic, I always believe in questioning authority. You shouldn’t rely on just one source of information. I follow American industry and other countries’ industries. I cross-check government statements and trust scientists and experts more in these matters.”
And if all goes according to plan, Özpolat notes, supply chain management’s role in a global vaccination effort will be so seamless that it’ll escape notice. “We don’t hear about supply chain when things are going right, but supply chains are global and interconnected. Supply chain management is a key skill.
“And in this instance, it’s directly related to the survival of our species.”

Professor Kerry LaPlante at the College of Pharmacy
‘A Sense of Duty’
Kerry LaPlante is a member of the Rhode Island Department of Health’s Rhode Island Vaccine Advisory Committee. The committee’s 20 members represent a wide range of expertise in medicine, pharmacy, ethics, advocacy, nonprofit management, education, and faith-based organizations. The group’s task is to develop a process by which a vaccine’s safety and efficacy will be evaluated, as well as advise the state Department of Health on how to prioritize the distribution of the vaccine equitably. This work maps exactly to LaPlante’s expertise.
LaPlante is a tenured professor of pharmacy at URI, an adjunct professor of medicine at Brown University, an infectious diseases pharmacotherapy specialist, and director of the Rhode Island Infectious Diseases Fellowship and Research Programs at the Veterans Affairs Medical Center in Providence. Her research expertise is in the treatment, outcomes, prevention, virulence inhibition, and decolonization of multiple drug-resistant bacteria. LaPlante has published more than 100 peer-reviewed articles and book chapters. Her laboratory has received funding from more than 50 research grants from the National Institutes of Health, the Department of Veterans Affairs, and Industry Investigator-Initiated Research.
“I am trained in safety and efficacy. I want to make sure the vaccine has an independent evaluation of efficacy and to ensure distribution is done in a fair and equitable manner,” LaPlante says. “I want to use my knowledge and expertise for public health decisions. I have a sense of duty as a Rhode Islander and as a pharmacist, and I’m glad it is acknowledged.”
After the public begins receiving the vaccine or vaccines, the FDA and CDC closely monitor adverse effects (side effects) to gauge the risks involved in getting vaccinated. Reports of adverse effects are collected by the Vaccine Adverse Event Reporting System, a national early warning system managed by the FDA and the CDC. And it doesn’t stop there. The CDC’s Vaccine Safety Datalink and the FDA’s Post-Licensure Rapid Immunization Safety Monitoring, two national healthcare organizations, as well as the Clinical Immunization Safety Assessment Project, a collaboration between the CDC and seven medical research centers, also monitor a vaccine’s safety.
If not already abundantly clear, determining which vaccine or vaccines might best serve Rhode Island’s 1 million residents requires the review of copious amounts of data—both recent and across history. There’s a wide range of science to consider in developing a vaccine, and with pandemic science, there’s going to be conflicting information, LaPlante says. She is involved in regular calls with the FDA and following research on persons with COVID-19 vulnerabilities. She’s studying adverse events, which can be different for every disease state reviewed. And LaPlante’s research doesn’t stop at the theoretical.
“The first thought I had was I must carefully review the data from the vaccines’ clinical trials,” she says.
In her role as an educator and researcher, LaPlante is committed to the plainspoken dissemination of knowledge. “We need to have science better communicated to the public. We need to do a better job,” she says. “I feel a strong sense of duty, a calling, and a responsibility to the profession of pharmacy to communicate and lead those discussions on safety and efficacy.”

Professor Virginia Lemay at the College of Pharmacy
‘The Human Factor’
The public’s participation is an essential factor in the success of a public health campaign. At least 60 percent of the population must be vaccinated for herd immunity to occur. So, a large adoption rate is crucial, and communication, critical. But as late as September, media outlets were reporting growing public mistrust of the FDA and a coronavirus vaccine. Ironically “vaccine hesitancy,” as the anti-vaccine phenomenon is known, is, like coronavirus, considered by the World Health Organization to be a global health threat.
Virgina Lemay, Pharm.D. ’00, clinical associate professor in the URI College of Pharmacy, precepts (directs) pharmacy students in community pharmacy-based clinical rotations focusing on medication therapy management, adult immunizations, diabetes, and proper selection of non-prescription, over-the-counter medication. She is director of the Post-graduate Year 1 (PGY1) Community-based Residency Program of the University of Rhode Island, whose residents focus on community practice, ambulatory care, and academia with the goal of becoming exemplary community pharmacists with highly developed clinical, analytical, and leadership skills.
Lemay, who has been published in many scientific journals, has been the recipient of numerous grants. Her scholarship focuses on clinical services provided by the community pharmacist in community pharmacy and ambulatory care settings. She has led her pharmacy students in targeted public health initiatives around diabetes and women’s health education, meningitis, HPV, and shingles vaccination.
Lemay envisions assisting in coronavirus inoculation when the vaccine becomes available. She recently submitted a proposal to the Institutional Review Board, commonly known as the IRB, for a survey on the topic of vaccine safety. It’s the first step in the process of planning a public health initiative, the information-gathering phase.

“We’ll assess the reluctance of people to receive the vaccine. It’s difficult to change a fixed mindset. From a social justice point of view, some people feel mistrustful. And there will always be that percentage of people who don’t want the vaccine,” Lemay says.
“Transparency is going to be critical. Without it, we’re going to create more mistrust. The problem is this is not something that can be addressed with just a soundbite. Right now, the eyes of the world are on the COVID vaccine. And getting vaccinated is a selfless act.”
When a vaccine is made available, priority will likely be given to certain demographics, but it’s not clear who will be the first in line to receive it. Some reports have said the priority will be first responders, then the elderly. Others have said the plan is first to inoculate the elderly, then first responders, youth 30 and under will be next in line, and then everyone else.
Lemay is most concerned about vulnerable populations. “Isn’t that what we’re about? Protecting the most vulnerable?” she says.
Last week Pfizer announced Rhode Island is one of four states it has chosen to pilot its vaccine. Pfizer will use the data gathered from its immunization pilot program to deliver, deploy, and administer its vaccine.
Lemay foresees pharmacists and URI pharmacy students fulfilling a vital role in battling coronavirus. A pharmacist dispenses knowledge alongside any vaccination or medication, Lemay notes. “Pharmacists are customer-service positions. We are constantly trying to provide clarity.
“That’s the human factor you bring to the science.”
—Marybeth Reilly-McGreen